In the May 2017 issue of Consumer Reports (CR), there is an article entitled Why the Best Insomnia Treatment Is Not a Drug. In earlier versions of their articles on sleep and medications for sleep they had reviewed various different sleeping agents but in this updated article they conclude that at best, the newer sleep medications add only between eight and 20 minutes of sleep time, and don’t improve how people feel or operate the next day.
They also reviewed a recent systematic research study by the federal Agency for Healthcare Research and Quality (AHRQ) that compared multiple treatments for sleep problems including drugs, cognitive behavioral therapy, and alternative therapies. This study concluded that cognitive behavioral therapy (CBT) is a safe and effective way to treat insomnia, and is more effective and safer than other treatments.
So Consumer Reports’ Best Buy drug pick is actually not a drug at all! It is Cognitive Behavioral Therapy (CBT). They recommend at least one session and optimally suggest three to six sessions of CBT with a psychologist.
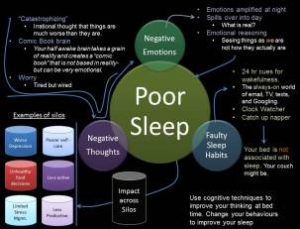
They also have a good description of how CBT works for insomnia. They explain how you meet with a psychologist and work on changing your beliefs about sleep, as well as changing certain behaviors that may contribute to insomnia. CR also includes a concise chart about bad sleep habits and how to fix them. They have an excellent description of CBT for insomnia here. If CBT was a sleep medication, promoted by a powerful drug company, it would be a multibillion-dollar product!
The bottom line for these articles was that Cognitive Behavioral Therapy for insomnia was safe, effective and long-lasting in its effects. What is clear from virtually every study of sleep treatments is that CBT may be the only treatment for sleep problems that doesn’t have side effects and negative impacts into the next day. According to a 2015 Consumer Report survey, 36% of people who took a sleeping pill felt drowsy the next day. They also report a study of 410,000 adults published in the American Journal of Public health which found that those who took sleeping pills were twice as likely to be in automobile crashes. The researchers in this study concluded that people taking sleep medications were as likely to have car accidents as people with blood-alcohol levels above the legal limit!
So what are the recommendations and interventions used in CBT for insomnia?
Spend only seven or eight hours in bed, and don’t compensate for insomnia by lying in bed for ten or eleven hours, as that just teaches you to be an inefficient sleeper.
Go to bed and get up at the same time every day.
Don’t go to bed unless you actually feel sleepy. If you can’t fall asleep get out of bed and do something peaceful and relaxing until you are sleepy, and then go back to bed.
Try to get regular exercise but don’t exercise in the evening.
Use your bed only for sleeping (or sex), don’t read or watch TV or look at your smartphone in bed.
Don’t nap.
Reduce your intake of caffeine, nicotine, and alcohol, especially later in the day.
OCD is a chronic psychological illness where a person has disturbing and recurring thoughts (obsessions) and compulsive behaviors that they repeat over and over.
OCD is at its core an anxiety disorder. The obsessive thoughts trigger intense anxiety, which the person attempts to ameliorate or reduce by either having compulsive behaviors or compulsive thoughts.
Typical obsessions that people have include:
thoughts about harming other people or being aggressive towards other people,
inappropriate sexual thoughts and feelings,
fear of germs or other types of contamination such as chemical contamination,
thoughts about symmetry and order,
taboo thoughts about religion or other “hot” issues.
Some typical examples of compulsive behaviors include:
Checking behaviors where the person repeatedly checks to see if the stove is turned off or a door is locked
Excessive cleaning, hand washing or showering
Counting behaviors
Arranging things in a particular and precise way
I’ve also written about hoarding, which is another type of compulsive behavior.
Some compulsive behaviors are actually thoughts, such as saying a particular prayer to yourself over and over.
A common type of OCD that I treat in my practice is germ phobia. The typical obsessive thought in these cases is that touching something such as the floor will transfer dangerous germs onto the person’s hands, which will then be transferred either to them or to someone they care about, causing great harm. These people are typically very fearful of public bathrooms and will avoid touching the doorknobs in them. In order to cope with perceived contamination, they will typically wash their hands many times a day, sometimes up to 30 to 50 times. When they cannot wash their hands they will use alcohol gel to sterilize their hands. Often the handwashing is so extreme that the person’s hands will look profoundly chapped and red.
When they feel particularly contaminated they will often take very long showers, washing and re-washing their body very carefully multiple times. These showers can take 30-60 minutes in some cases.
Exposure and Response Prevention Treatment (ERP) for Contamination OCD
OCD that is accompanied by clear rituals such as handwashing is easily and effectively treated using a Cognitive Behavioral Approach that focuses on something called Exposure and Response Prevention (ERP). Let me describe a hypothetical case. (This is a hypothetical case that may include composite aspects of clients I have treated, with all identifiable client information changed.)
Susana came to me because she had developed a very severe case of contamination OCD. Her primary fear was that by touching something that might have germs, she would transfer these germs to her children, husband, or even to strangers, and that they would sicken and die. As a result of these fears, she would wash her hands more than 50 times a day, and take showers that lasted more than an hour during which she would scrub up and wash down three or four times.
She also had developed almost complete avoidances of many situations. Public restrooms terrified her, so she could not leave the home for long periods of time. She was afraid of contaminating her car, which then might contaminate people she loved, so she avoided driving. Work was out of the question since she was spending hours a day on OCD rituals.
The first step was to thoroughly evaluate her OCD. I gave her multiple questionnaires that evaluated the frequency of obsessive thoughts, compulsive behaviors, and avoidant behaviors. The same questionnaires also evaluated the level of anxiety and distress caused by both the obsessions and the compulsions. This gave us a good baseline set of numbers that described the state of her OCD. As part of the same evaluation, I obtained detailed information about all of the things that she was avoiding doing.
The next step was to do some Cognitive Behavioral Therapy (CBT) on her belief systems about germs and contamination. This consisted primarily of a set of conversations where I asked open-ended Socratic-style questions about her beliefs. She showed a variety of common OCD distorted thoughts and beliefs.
Common Thought Distortions in Contamination OCD
All germs are lethal and deadly: This distortion is basically the belief that every microorganism causes serious or fatal diseases. It’s actually not true. We are surrounded by bacteria, and most of them are harmless or even beneficial. The most common kind of harmful germs or viruses are the common cold and the flu. Neither these illnesses are particularly dangerous although they are unpleasant. More dangerous germs such as HIV or tuberculosis are extremely rare in developed nations, and the virus that causes HIV is extremely fragile and cannot survive for more than a couple of minutes on most surfaces.
Germs live forever on any surface: This is the belief that once a germ attaches itself to a surface it will stay there forever and be capable of infecting you. In reality, most surfaces are fairly inhospitable for bacteria and viruses, and the microorganisms become inactivated fairly quickly, usually within minutes or at most an hour.
Things transfer at 100% potency: The law of transfer says that with each transfer the potency of what is being transferred becomes less and less. So if you touch something that has germs on it, your hand will have some germs transfer. If you then touch something, such as a computer keyboard, fewer germs will transfer. Then when someone else touches the keyboard, even fewer germs will transfer to them. The more transfers the less is transferred.
Humans have no immune system: This is the belief that every germ or virus that one contacts will cause illness. Humans actually have a very robust immune system. Every day our immune system kills off a variety of germs and viruses we get exposed to. Unless we are exposed to many germs or viruses, our immune system usually does a good job of resisting illness.
The Treatment: Using Exposure and Response Prevention
We did some experiments to test her beliefs. One experiment I like to do is the chalk dust experiment. I have the patient touch some chalk dust, and then they touch my hand, and then I touch my keyboard of my computer, and then I have them touch the keyboard with a clean hand. Thus they graphically see that each transfer moves less and less chalk dust to the next item.
We spent a few sessions discussing and correcting the misconceptions about germs and illness. This began the process of getting ready to start the essential part of the treatment, Exposure and Response Prevention. (ERP)
To prepare for ERP we first made a laddered list of things that would be scary for her. The list went from fairly easy tasks which were a little scary, to tasks that would be terrifying. We rated the anxiety on a 0-10 scale.
I asked her to pick a task that would be somewhat challenging but not terrifying to start with. She picked a task with moderate fear attached to it, touching the floor of my office (which is a carpeted floor.) I also told her that anything that I would ask her to do I would also do with her.
I had her rub both hands on the carpeted floor. Then I asked her to just sit with her anxiety. Initially, her level of anxiety was 10 out of 10. I asked her to narrate her thoughts. “My hands are covered with dangerous germs,” she said.
Over 15 minutes or so her anxiety began to diminish. It went down to about a 7. I noticed that she was holding her hands in the air, so I asked her to put them on her lap. This increased her anxiety briefly, but after a few minutes he anxiety came back down to a 7.
Over another 20 or 30 minutes, her anxiety came down even further. Now it was only a level 4. I asked her to describe her thoughts. “Your carpet probably isn’t really covered with very many germs, and therefore my hands probably don’t have very many germs on them,” she said.
Then I asked her to do something a little bit more challenging – to rub her hands on her face. This made her anxious, but she did it, and after a few minutes of higher anxiety the anxiety subsided again.
By the end of our official face-to-face session, her anxiety level was a 3 out of 10. I asked her if she had any alcohol gel or cleanser in her purse, which she did, and I asked her to leave that in my office. Then I asked her to spend at least another 30 minutes in my waiting room to see if the anxiety level would come down even further, without washing or cleansing her hands. At the next session, she told me that the anxiety level had come down to a level 2, which amazed her given that she had started at 10. I had asked her not to wash her hands for several hours which she did.
At the next session, we tackled another item on her list, the ATM. She was afraid to touch ATMs with her fingers, and either used the back of her knuckles or used alcohol gel after touching the ATM. So we went next door to the local banks ATM, and I had her repeatedly touch the keys with her fingertips. This brought her anxiety level up to about 7, so we kept repeating the task until the anxiety began to subside. Once again I asked her not to wash or use alcohol gel.
A few sessions later after using exposure and response prevention on a variety of other issues, we tackled the top of her list – the public restroom! For many contamination OCD patients, this is the ultimate challenge. We went next door to the building’s restroom, where I put a sign on the door, Closed for Maintenance. Next, I modeled touching the doorknob, the sink, and she did the same. We went back to my office and once again she sat with her anxiety until it came way down.
Once her anxiety had dropped we went back into the restroom and did a harder task. First I modeled touching the toilet seat, and then she touched it. Not surprisingly this raised her anxiety very high. Once again we went back to my office and she sat with that anxiety. We discussed the nature of what toilet seats are made of, and how long germs could live upon them. Gradually her anxiety diminished to about a level of 5, which was a large drop for her.
Between sessions, I asked her to practice these tasks on her own. I explained that the key was to sit with the anxiety for a long enough time for it to subside naturally without any hand cleaning or sterilization. She practiced on a daily basis and made rapid progress on the items we had done together and some other items that were also on her feared list.
By this point, she had lowered her hand washing from 40 or 50 times a day to only several specific situations. After using the toilet, before preparing food, and after preparing food. She had stopped using alcohol gel completely.
A few months later she began to look for work for the first time in several years, as her OCD was virtually completely resolved. I continued to see her intermittently over the next few years, and her OCD continued not to be a problem, although there were some other non-OCD challenges.
In Part Two of this article, I will discuss the use of medications for the treatment of OCD, Thought OCD, Checking OCD, and Health OCD.
The New York Times had an interesting article about how depression is often misdiagnosed in the US, and how most people who actually have depression don’t get treatment. They reference a research study just published in the JAMA Internal Medicine.
This research study performed by Mark Olfson, Carlos Blanco, and Steven C. Marcus, looked at responses from 46,417 people on the Patient Health Questionnaire-2 (PHQ-2) which is a brief screening tool for depression. A score of over 3 indicates depression on this scale.
What did they find? They found that approximately 8.4% of all adults studied had depression, but only 28.7% had received any depression treatment in the previous year! That means 71.3% of the people who suffer depression got no treatment for this depression.
Of those who were being treated for depression, about 30% actually had depression based on the screening, and another 22% had serious psychological distress. That means that of the people in the study who were being treated for depression roughly 48% neither suffered depression nor did they suffer serious psychological distress, indicating inaccurate diagnoses by the treating professionals.
There were some interesting correlates of depression. About eighteen percent of those in the lowest income group suffered depression, while only 3.7% of those in the highest income group suffered depression. It pays to be rich!
Depression was more common in those who were separated, divorced, widowed, or who had less than a high school education. None of this is terribly surprising.
How did depression sort out by age?
In the 18 to 34-year-old group 6.6% suffered depression. In the 35 to 49-year-old group 8.8% suffered depression. Ten percent of the 50 to 64-year-old group suffered depression. Of those over 65, only 8.3% suffered depression. So at least in this sample the 50 to 64-year-old group was slightly more likely to suffer depression, and contrary to what many people think, the youngest adults were somewhat less likely to suffer depression.
Of those who were married only 6.3% suffered depression. Of those who were separated, divorced, or widowed, 13.3% suffered depression. Divorce is bad for mental health, with almost a doubling of rates of depression.
Most of the patients who were treated for depression were treated by general practitioners (73%), with roughly 24% receiving treatment by psychiatrists and 13% receiving treatment by other mental health specialists. (There was some overlap, that’s why the numbers add up to more than 100%.) This may explain the rather poor diagnosis and treatment of depression because general practitioners although competent and intelligent, are very busy and typically only have a few minutes to spend with each patient, not enough to do a good job diagnosing and treating depression.
CONCLUSIONS ABOUT DEPRESSION FINDINGS
What can we conclude from this research?
Almost 10% of the adult population suffers from depression. Of those people who have depression less than 30% of them will get any treatment for depression.
You are more likely to suffer depression if you are in the lowest income group, divorced, separated or widowed, or have no high school education. If you are married you have half the probability of being depressed.
Many adults receive depression treatment even though they don’t really meet the criteria for depression. In this study, almost half of the people receiving treatment for depression were neither depressed nor were they even particularly distressed.
Rates of depression by age groups were relatively equal, with the youngest age group having the least depression and the middle-aged group (50 to 64) suffering somewhat more depression. Married people are suffer half as much depression as divorced, separated, or widowed people.
Most people received depression treatment from their general practitioner or internal medicine doctor, with a smaller number receiving treatment from a psychiatrist, and even a smaller number receiving treatment from psychologists. This also meant that most people who receive depression treatment were treated using medication, and very few people received psychotherapy, even though most studies comparing medication to cognitive behavioral therapy for depression have shown that therapy performs at least as well as medication and probably better over the long term, with less relapse.
Reading between the lines of this study, it suggests that many people who feel depressed would benefit from receiving an accurate diagnosis from a clinical psychologist, and might very well also benefit from receiving cognitive behavioral therapy for depression rather than medication. Even if medication is indicated, a psychologist could recommend it to the patient’s general practitioner, and then monitor more closely the results.
The study also suggests that many people receive antidepressant medication who actually are not depressed, which needlessly exposes them to side effects and also fails to provide the correct treatment for what troubles them.
And finally, since only about 30% of those who suffer depression received any treatment for it, if you feel depressed, be sure to pursue treatment for depression. Get an accurate diagnosis and then get treatment, ideally with a psychologist or therapist who practices cognitive behavioral therapy. If you want more information about depression, I’ve written extensively about it with a complete list of depression articles.